Assessment
ProblemIs the problem a priority? | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Judgement | Research evidence | Additional considerations | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
The Atlas of MS estimates there are 2.8 million people living with multiple sclerosis (MS). Of these, 11% have progressive forms of MS. There is unequal access to DMTs globally, with 14% of countries not having access to any on-label disease-modifying therapies (DMTs). Low income countries (LICs), lower middle income countries (LMICs) and upper middle countries (UMICs) are affected more than high income countries (HICs). Treatment options for people with progressive forms of MS are often limited, and DMT regulatory approvals and indications are sometimes restricted to active forms of PMS. Evidence for both on-label and off-label DMTs should be considered when considering essential medicines for MS.
PICO 4: The Panel decided to review DMTs for active and/or progressing forms of progressive MS to consider the most appropriate treatment approach.
PICO 5: The Panel decided to review DMTs for not active and not progressing or indeterminate forms of progressive MS to consider the most appropriate treatment approach.
PICO 6: The Panel decided to review DMTs for active and/or progressing forms of progressive MS when there is a lack of treatment response to consider the most appropriate treatment approach.
Panel members with COI for DMTs reviewed for PMS: Anthony Traboulsee, Jagannadha Avasarala, Carlos Navas, Maya Zeineddine, Riley Bove, Dina Jacobs, Shanthi Viswanathan, Bassem Yamout, Kathy Costello.
Undetermined COI: Hans-Peter Hartung. | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Desirable EffectsHow substantial are the desirable anticipated effects for each intervention? | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Judgement | Research evidence | Additional considerations | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
The evidence base on DMTs for progressive forms of multiple sclerosis (PMS) was retrieved through systematic reviews of the biomedical literature developed according to the Cochrane methodology. The search was performed on February 11, 2022. Included studies were randomised-controlled trials (RCT). Thirty treatments (with registered indications for MS, as well as non-licensed but used off-label in clinical practice) were included in a network metanalysis, compared vs placebo or vs any other DMT. Direct, pairwise comparisons were assessed assuming placebo as the common comparator. Among people with PMS, three populations were identified by the panel: with active PMS, with non-active PMS and with active PMS when there is a lack of treatment response (switching). We retrieved 23 RCTs (10,167 participants in total) eligible for analysis, one of which reported no outcomes of interest (Etemadifar 2019). No study included only people with non-active disease or people with active PMS and lack of treatment response. Eighteen RCTs included only people with active PMS, 3 RCTs included a mixed population and in 2 RCTs the PMS phenotype was not reported. We performed an overall analysis including all RCTs and a sensitivity analysis including only the 18 studies with active forms of PMS. However, such analysis could not include pivotal RCTs of treatments that were considered very important by the panel (among them the pivotal trial of the only DMT licensed for the treatment of primary progressive MS). Therefore the panel agreed in considering as the evidence base the analysis including all retrieved RCTs. The resulting heterogeneity was considered acceptable by the panel, given the limited proportion (17%) of participants included in trials with a mixed population. Among the desirable effects, most studies assessed disability and relapse at 24 months. No study assessed cognitive decline. Disability at 24 and 36 months was reported in 11 and 5 studies, respectively. Point estimates were mostly in favor of the intervention compared to placebo. However, the certainty in such estimates was lowered by imprecision. Frequency of relapse was reported at 12, 24 and 36 months in 1, 6 and 4 RCTs, respectively, with interferon beta products and azathioprine providing estimates significantly better than placebo, although with moderate to very low certainty due to imprecision. Interferon beta products, siponimod and fingolimod showed higher efficacy than placebo in regard to new gadolinium-enhancing T1-weighted MRI lesions and new or enlarging T2-weighted MRI lesions at 12, 24 and 36 months. Certainty in MRI outcomes was overall better than the other outcomes due to lower imprecision of the point estimates. Quality of life was assessed in three RCTs on interferon beta 1a, natalizumab and ocrelizumab, reporting point estimates favouring treatment vs placebo, although with moderate to low certainty due to imprecision.               | Due to the complexity of the network meta-analysis, only randomised controlled-trials (RCTs) were assessed. There is a considerable number of non-randomised controlled studies that may also provide important insight to comparative effectiveness. In light of the complexity of the methodology, it was not feasible to systematically assess and consider these for the recommendations. The panel noted that different outcomes and different number of outcomes for desirable effects had been measured in the trials, and therefore the evidence between DMTs was not easy to compare. As the understanding of PMS has evolved, the trials are reporting different outcomes. For ocrelizumab, the focus in the PPMS trial was on disability progression, MRI lesions and brain volume loss, but not relapses. Relapses were measured in the two relapsing MS trials for ocrelizumab, but with annualised relapse rate (ARR). ARR did not meet outcome inclusion criteria, so the effect of ocrelizumab on relapses is not included in either the PMS or RMS analyses. Furthermore, differences in trial design and being unable to include some outcomes in the NMA resulted in fewer outcomes being included for some DMTs compared to other DMTs. Please see 'balance of effects' for more details. Most studies consider disability, newer studies measure MRIs and QoL, none looked at cognitive decline. Most prominent desirable effects found in T1-and T2-weighted MRI lesions with moderate and high certainty of evidence. All treatments with this outcome showed desirable effects with moderate or high certainty. A number of studies looking a QoL, some with moderate certainty, in favour of treatment. Mortality in favour of treatment, but event numbers very small. The panel noted that for non-active populations and when switching due to lack of treatment response, the evidence is indirect. | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Undesirable EffectsHow substantial are the undesirable anticipated effects for each intervention? | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Judgement | Research evidence | Additional considerations | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Among the undesirable effects, serious adverse events (SAEs) were reported by 15 studies, while mortality and discontinuation due to adverse events were reported by 21 studies. For the latter, two studies reported no events in either arm and were excluded from analysis. Certainty of the evidence relative to SAEs was very low for most treatments, mainly due to imprecision of the estimates.    | The panel noted that for some DMTs no SAEs were reported due to data extraction having specific inclusion criteria. It is important to distinguish 'no data' from 'no SAEs'. For example, azathioprine had a large amount of discontinuation events, but there were no data for SAEs. This is because a very specific definition of SAEs was used for the analysis, so for studies that did not use that classification, the data could not be extracted as severe adverse events. Two issues were noted: (1) Only ‘discontinuation due to any cause’ were included in the net sum as also including ‘SAEs’ would have double-counted these events. (2) The panel noted there were concerns with post-marketing surveillance from a safety standpoint. Some of the DMTs have SAEs, albeit rare, e.g. risk of PML for natalizumab, fingolimod risk of cardiac issues and infections that were only captured in post-marketing surveillance and not in the original RCTs. The panel noted that, while the judgement of undesirable effects as ‘trivial’ is in line with the RCT data reviewed, this is not the view of clinical practice due to post-marketing sureveilance. The panel also highlighted discontinuation of DMTs for risk of rebound of MS disease activity that prompted a warning for S1P modulators (fingolimod) and natalizumab. Rebound phenomena can be as high as 10% with S1P modulators. The panel highligted that in the NMA only RCTs are considered, so post-marketing studies and surveillance are not included. There was not capacity within the scope of this project to systematically review all post-marketing studies for all the DMTs. The panel decided that post-marketing safety warnings will be used to contexualise the EtD. EMA safety warnings and label changes can be found here: Summary of extra safety considerations: 1. Natalizumab: updated PML risk for JCV positive patients identified in post-marketing safety studies. 2. Fingolimod: rebound effect and cardiovascular, liver and cancer risks identified in post-marketing safety studies. | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Certainty of evidenceWhat is the overall certainty of the evidence of effects for each intervention? | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Judgement | Research evidence | Additional considerations | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
All treatments showed a very low certainty of the evidence in at least one outcome, manly due to imprecision of the estimates, therefore the overall certainty is always very low. Note on deviation from standard GRADE methodology: After assessment of certainty overall, the panel looked across all individual outcomes of all DMTs and considered whether there was less concern for imprecision, based on the trend on certainty levels and direction of the individual outcomes. The panel decided to downgrade less for imprecision for the overall assessment for interferon beta 1a, siponimod and fingolimod. | The panel raised concerns around the methodology of assessing the balance of effects. Firstly, there are limitations in the use of health state utility values (HSUVs), as these have not been validated for MS and also lack specific input by people with MS (pwMS). Secondly, the addition of outcomes to derive a summary figure for the balance of effects is complex due to the heterogeity of the studies included. Studies that measure more desirable outcomes may look better than those that measure fewer or different outcomes. Please see 'balance of effects' for more details. The most frequent reason for downgrading the certainty of evidence came from imprecision (rather than risk of bias or indirectness) from very large confidence intervals that crossed the thresholds of trivial, small, moderate and large effects. The overall certainty considers the lowest certainty of evidence of the outcomes included. The panel noted that this has made all the evidence very low certainty of evidence. This is making it challenging to differentiate between DMTs. If considering multiple outcomes and they are all in the same direction, e.g. showing benefit, this would decrease concern for certainty of evidence for imprecision. The panel decided to consider this approach to create more granularity in the assessment. Summary: adjustments of less downgrading for interferon beta 1a, siponimod and fingolimod. | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
ValuesIs there important uncertainty about or variability in how much people value the main outcomes? | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Judgement | Research evidence | Additional considerations | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Health State Utility Values We conducted a scoping review to retrieve the available evidence on Health State Utility Values (HSUVs) for MS. Health utility is a summary index measure of health-related quality of life, usually obtained by means of surveys among people affected by a condition. HSUVs are used to assign a value to health states on a scale on which 1 is equivalent to full health and 0 is considered equivalent to being dead. Values can also be negative, representing health states values worse than being dead. We considered eligible any systematic review, overview of reviews, or Health Technology Assessment (HTA) report. If such studies were not available, we searched for studies designed to specifically collect Health-Related Quality of Life data, or as part of an RCT or prospective observational study. The search was performed from January 2010 to February 2022 on MEDLINE, Embase, Web of Science Core Collection, the Health Technology Assessment Database, and Epistemonikos databases. We retrieved 1,170 citations. After screening of titles and abstracts, detailed assessment of eligibility was performed on 8 reviews (including a report from the Institute for Clinical and Economic Review providing data on utilities values based on previously published studies) and 11 primary studies. Data on HSUVs were extracted from four systematic reviews (Chataway 2021, Naci 2010, Zhou 2021, Prevolnik Rupel 2019) and one evidence report (ICER 2017). We also checked all the individual studies included in the 4 systematic reviews. After considering any generic QoL measures, only studies using the EQ-5D tool as the primary outcome measure were appraised to assess QoL among pwMS. This choice was based on the amount of work that has been done about the EQ-5D and its measurement properties. Moreover, it is a commonly used generic QoL instrument that allows for direct derivation of the value a person places on their life at the time the outcome is assessed. Therefore EQ-5D was considered as the most direct measure of QoL among PwMS. Three reviews (Wittenberg 2013, Ngorsuraches 2021, Milinis 2016) were excluded because the topic addressed was not relevant for our aim. Of the 11 individual studies retrieved, two (Hawton 2016, Erikkson 2019) were already included in one systematic review (Chataway 2021); five (Krokavcova 2019, Goodwin 2018, Ahmad 2020, Ahmad 2021, Ahmad 2017) used scales differnt from the EQ-5D and four (Hernandez 2021, Hawton 212, Hawton 2012 A, Goodwin 2019) addressed topics that were not pertinent. Our review identified published evidence only for some of the outcomes voted as critical or important by the panel, since most studies reported HSUVs related to being affected by MS in general. Some studies did not even report the type of MS (relapsing or progressive). Another limitation of the available evidence is that most studies were conducted in high-income countries (HICs) and none were conducted in lower-middle or lower income countries. Namely, for the outcomes "QoL impairment" and "relapse" we found evidence in the Chataway 2021 review, including studies assessing the impact of such outcomes on QoL by means of the EQ-5D tool. For the EDSS- based "Disability " outcome voted by the panel as critical, HSUVs were available for different EDSS scores (6, 7 and 8). Having to choose one utility value for this outcome, the panel agreed to consider the HSUVs related to an EDSS score of 6, based on the following considerations: - "disability worsening" is a dichotomous outcome (N of patients with the outcome) and the adopted definition of it is: "an increase of 1 EDSS point in participants with a baseline score up to 5, or of 0.5 points for participants with a baseline EDSS ofover 5.5". Therefore, the former includes all cases where the worsening was up to 6. The latter, includes all people with an EDSS score of 6 or higher. - the EDSS is highly centered on walking ability (EDSS 5.5= Able to walk without aid or rest for 100m ; EDSS 6.0= Requires a walking aid – cane, crutch, etc. – to walk about 100m with or without resting) - the numerical difference between the HSUVs of EDSS 6 and 7 is small - An EDSS score of 8 refers to people " Essentially restricted to bed or chair or pushed in wheelchair. May be out of bed itself much of the day. Retains many self-care functions. Generally has effective use of arms". Some of such patients may not have been eligible for inclusion on pivotal trials on DMTs that we are evaluating. As per the outcomes "New gadolinium-enhancing positive T1 weighted MRI lesions", "New or enlarging T2 weighted MRI lesions", "Serious Adverse Events" and "Discontinuation of treatment due to adverse events (tolerability)", no evidence was retrieved, and the panel agreed on assumed utility values. We did not find any RCT assessing the outcome "cognitive decline". Also "Mortality" was voted as a critical outcome by the panel, and its utility value - as mentioned above - is zero. References
Patients' preferences and values Visser 2021: An online survey to elicit patient preferences for attributes of MS therapies in three Western European countries (the Netherlands, France, and the United Kingdom). Some attributes and attribute levels concerning MS treatment were derived from systematic literature reviews and were verified during two focus group sessions with pwMS. Respondents had to repeatedly choose between various treatment scenarios with four treatment outcomes: risk of relapse, reduction of disease progression, risk of side effects and mode of administration. Based on the preferences of 753 pwMS, two classes were identified Patients in class 1 generally preferred: • any treatment over no treatment. • A treatment to provide less risk of relapse and less disease progression. • Rare severe side effects were less desirable than very common mild side effects. Moderate side effects were perceived not statistically different from very common mild side effects (p = 0.427). • one pill per day was most preferred followed by an implant replaced every year, an implant replaced every three years, two pills per day, and injections once per week. Patients in class 2- preferred: • no treatment. • a lower risk of relapse and reducing disease progression • rare severe side effects were less desirable than very common mild side effects • indifferent between common moderate side effects and very common mild side effects (p = 0.169) • pills twice per day vs implants, whereas injections once per week were not statistically different from the reference level injections three times per week (p = 0.396) In general, in both classes’ patients preferred their treatment to reduce risk of relapse and disease progression, and the presence of rare severe side effects had a negative effect on treatment choice as compared to very common mild side effects. Preferences for modes of administration differed per class, but it was observed that patients generally would be open to having an implant as a mode of administration. Patients were willing to accept an increase in risk of relapse and some disease progression to get their treatment via an implant rather than via injections. Furthermore, the mean predicted uptake was the highest for the implant, followed by pills, injections, and no treatment. References Visser LA, Huls SPI, Uyl-de Groot CA, de Bekker-Grob EW, Redekop WK. An implantable device to treat multiple sclerosis: A discrete choice experiment on patient preferences in three European countries. Journal of the Neurological Sciences. 2021;428:117587. Protocol: https://osf.io/5edjf | The panel noted concerns around the accuracy and validity of the HSUVs used for the calculations. There is a lack of evidence for the prioritised HSUVs, especially from the perspective of MS and with input from pwMS. The panel considered there to be significant differences between MS and other disease areas, e.g. due to the young age of pwMS, cognitive decline may be valued very differently among pwMS compared to people with Alzheimer disease. For a number of HSUVs used in the analysis the panel had to estimate an appropriate value based on other MS outcomes. Whilst it was recognised that the methodology was useful as a tool, it should be interpreted with caution, especially in absolute terms.
The panel noted the lack of evidence also for the systematic review on values and preferences for pwMS. The evidence suggested that the order of prefrence for mode of administration was oral, infusion, injections, and that frequency of administration was an important factor. The panel noted personal and anecdotal evidence of infrequent infusions sometimes preferred over frequent oral medication.
The panel judged whether there was important uncertainty in how much people valued the main outcomes without consideration for the HSUVs and thresholds.
All DMTs were judged as "probably no important uncertainty or variability". | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Balance of effectsDoes the balance between desirable and undesirable effects favor the intervention or the comparison for each intervention? | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Judgement | Research evidence | Additional considerations | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Assessing the balance of effects implies judgement. In order to make this process transparent, and noting the complexity generated by a considerable number of outcomes and of interventions to assess, MEMP attributed to each outcome a numerical value (health state utility value (HSUV)) ranging from 0 to 1, where 0=death and 1=full health. Values lower than zero indicate a health state that is considered as worse than being dead. A set of outcome-specific HSUVs, one for each of the critical and important outcomes identified by MEMP, was developed through the following steps: - the evidence review team performed a scoping review of the literature, retrieving 8 reviews (including an evidence report from the Institute for Clinical and Economic Review, ICER, providing data on utility values based on previously published studies) and 11 primary studies. on quality of life (QoL) of people with MS expressed as HSUVs. Detailed assessment was performed on four systematic reviews (Chataway 2021, Naci 2010, Prevolnik Rupel 2019, Zhou 2021) and one evidence report (ICER 2017) measuring QoL by means of the EQ-5D scale, that was considered as the most direct measure of QoL to assess quality of life among persons with MS and it is a commonly used generic QoL instrument allowing for direct derivation of the value a person places on their life at the time the outcome is assessed. (more details about evidence retrieval and selection can be found in the above section "Values"). - each study included in the retrieved systematic reviews was assessed and HSUVs were extracted and shared with MEMP. Unfortunately, most studies provided non-outcome-specific HSUVs, generally related to being affected by MS, therefore - to obtain a list of outcome-specific HSUVs - most values were assumed by the panel. - each outcome-specific HSUV was combined with the point estimate of the absolute risk reduction per 1,000 (and its 95% confidence intervals (CIs)) for that outcome reported in the clinical trials on efficacy and safety of DMDs included in the network metanalysis that MEMP referred to as the evidence base. Such combination of HSUVs and absolute risk reduction (or increase, in case of undesirable effect) estimate was performed by means of a formula based on an international stakeholder survey of thresholds according to disease conditions & HSUVs (Morgano et al., in preparation), according to a new method being implemented by the GRADE Working Group. - the resulting point value (and its 95% CIs) was contextualised within a range of magnitude of effects structured as "trivial", "small", "moderate" and "large", separated by specific thresholds. - the imprecision of such point value was determined by the width of its 95% CIs: one level downgrading for each threshold crossed by the CIs. Downgrading for imprecision was possible up to three levels (e.g. from "high" to "very low") The table shows the net balance of effects for DMTs in PMS, resulting from combining desirable and undesirable effects of each drug. Details about thresholds between the four magnitudes of effect ("trivial", "small", "moderate" and "large") can be found here: https://www.msif.org/wp-content/uploads/2022/09/Balance-of-effects-calculations-net-balance.xlsx The column "Number of outcomes" reports how many outcomes were considered by MEMP to calculate the net balance of effects, among those available for each drug in the RCTs retrieved through the systematic review and NMA that served as the evidence base. In order to obtain pooled network estimates allowing comparisons among the available treatment alternatives, for each outcome only one measure of effect was necessarily chosen (e.g., the predefined outcome measure for "relapse" was dichotomous: "number of patients with a relapse"). As a consequence, for some of the drugs, not all the data relative to the reported outcomes were extractable and usable for analysis (e.g. trials where relapses were expressed as "annualized relapse rate" - continuous outcome measure - were not extractable and are not reported in the table). Therefore, the number of important or critical outcomes differed by different intervention due to varying outcomes included in trials (e.g. Drug A had 8 included outcomes, Drug B had 3 included outcomes). The panel noted that this impacted the quantitative benefits and harms across outcomes, but the plain number of outcomes for each drug per-se was not considered as informative for the MEMP decisions. The ranking provided a starting point for discussion when considering the balance of effects, but the approach and limitations needed to be considered carefully when contextualising the information for making recommendations. To illustrate this point, see the two interferons, 1a and 1b. From the range of outcomes included, 1a has a large benefit for desirable effects, whereas 1b has a moderate benefit. Yet if the sum only included outcomes common to both DMTs (relapses and disability), 1b would still have moderate benefit, whilst 1a would show trivial harm. The reason 1a achieves the large benefit overall is through having data for additional important outcomes, for quality of life and MRI lesions. Table Summary net balance of effects with net health state utility values (HSUVs) of DMTs in PMS.  References
| The panel decided to take the following approach to avoid duplication between outcomes in HSUV calculations: If two time-points are measured, only the one with higher certainty is used. If the certainty is the same, the longer time-frame is used. If both serious adverse events and discontinuation due to adverse events are measured, only discontinuation due to adverse events is used. The panel noted that the methods suppress the certainty for all DMTs to very low. However, within the ‘very low’ there are still different levels of certainty. Please note certainty rating adjustments for interferon beta 1a, siponimod and fingolimod. Imprecision is a challenge in the field with small studies and outcomes with high variability or ‘soft’ (e.g. EDSS) outcomes. More research is needed. Panel members felt additional uncertainty related to the very small trials for two treatments: azathioprine (n=67) and methotrexate (n=60) and questioned whether they should be considered at all in the assessment. The panel questioned whether these trials were adequate to make any recommendation. Previously highlighted issues around the accuracy of the summary value and net balance were noted by the panel, e.g. ocrelizumab was assessing PPMS and did not include relapses, which affects its overall score. Shortlisting Laquinimod was excluded as it shows net harm. The panel debated whether DMTs with small trials should be excluded (some MS trials are 25x larger). However, imprecision is affected by many factors, number of participants is only one. The DMTs with only small RCTs were retained in the assessment. The panel decided to assess DMTs from azathioprine to ocrelizumab for the full EtD. Ocrelizumab is the only DMT with regulatory approval for PPMS. The panel noted that we are not comparing the relative efficacy and safety risks, but combining this with HSUVs and the other outcomes, including the number of outcomes. -- Judgements on shortlisted DMTs The panel judged the DMTs with very low certainty of evidence as 'probably favours treatment'. Ocrelizumab, despite its small benefit was judged as ‘probably favours intervention’ as the trial looked at PPMS and did not measure relapse as an outcome, i.e. when the outcomes are summed-up, it is more difficult to reach net benefit. Siponimod was judged to favour the intervention due to higher certainty ('low' rater than 'very low') and apparent higher net effect than interferon beta 1a and fingolimod, despite them also having low certainty of evidence. The exact ranking of the DMTs should be analysed with caution, because the panel noted that certain medicines had a greater number of prioritized outcomes measured (e.g. interferon beta 1a featured 7 outcomes, other DMTs featured 3 or 4). For medicines with more outcomes this may increase our certainty, but also results in a larger contribution to the net balance than medicines that do not have as many outcomes reported. | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Resources requiredHow large are the resource requirements (costs) for each intervention? | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Judgement | Research evidence | Additional considerations | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Long-term resource requirements are influenced by the DMTs patent status around the world. Patent landscape of DMTs available here: http://www.msif.org/wp-content/uploads/2022/03/DMTs-patent-overview-March-22.pdf Evidence on cost of DMTs for PMS was retrieved from manual search of grey literature (publicly available price databases, non-commercial, governmental agencies, HTA reports). We collected the prices of DMTs used in PMS considering both originators and generics/biosimilars, when available, with registered indication for PMS as well as off-label. Whenever an alternative was available we chose the lowest price. Prices are compared by means of their yearly cost per patient. This was calculated from the cost of one drug unit (tablet, pre-filled syringe, etc.) multiplied by the number of units administered yearly, according to the recommended dosage. Whenever available, ex-factory (“ex-work”) price was reported, without taxes and duties/fees for distribution by the pharmacies. All prices are expressed in US Dollars by conversion from the original currency. Most data are available from HICs that also show a wider availability of DMTs. Since MEMP has a particular interest for low-resource settings in lower income countries, we reported only three HICs (one from southern and one from northern Europe, and the US) and focused mainly in searching information from UMICs, LMICs and LICs. We found no data from the latter. The following drugs, originally included in the MEMP PICO questions, are not included in the cost comparison tables: leflunomide, diroximel fumarate, fludarabine, minocycline, mycophenolate mofetil, monomethyl fumarate (no evidence from RCTs was retrieved); laquinimod (no price information was retrieved) Table 1 reports the price and Divided Daily Dose (DDD) of DMDs used in MS already included in the WHO EML. Table 2A summarizes median prices of each DMD for each patient per year across country incomes. Tables 2 to 4 show details about the drug price in each country and the cost per-unit and the price per patient per year (unit price multiplied by the number of units administered yearly). together with the source of each information. Prices from years before 2020 are not adjusted for inflation to 2022 values. The lowest reported price of each drug across each country income class is in bold green color; the highest in bold red. Abbreviations are listed below after the tables. If comparing drug prices for relapsing and progressive MS in the "Resources Required" domain, please note that price assessment for progressive MS was based on currency exchange rates of April 12, 2022, while price assessment for relapsing MS was performed on June 6, 2022. Therefore some differences may be appreciable. General considerations Data from price databases suggests that DMT prices are generally higher in HICs, particularly in the US, where they often are multiples of the prices in other HICs. In UMICs, and particularly in LMICs, they are on average lower, although with notable variability. The DMTs with the lowest median price/year/patient in the considered HICs are cyclophosphamide and azathioprine, while in the considered UMICs and LMICs it is methotrexate. The DMTs with the highest median price/year/patient in the considered countries, regardless of the income, are immunoglobulins. Generally, older, out-of-patent drugs show lower prices and also lower price variability, while branded drugs often show a remarkable variability, the highest prices being in the US among the HICs, Lebanon among the UMICs and Morocco among the LMICs. Such variability may be in part explained by the healthcare system organisation (insurance-based rather than universal coverage) and by negotiations between the local government and the producers, that are usually confidential and may result in a substantial reduction of prices, sometimes > 50%. Discounts may have various determinants, such as price-volume agreements, presence on the market of short expiry products creating competition, and others. The only countries for which we reported a negotiated price are Turkey (that adopted a negotiation based on a fixed currency exchange with EUR) and one LMIC remaining confidential. One more determinant of variation in prices may be different timings in patent expiry (e.g. fingolimod, still branded in the EU but generic in other extra-EU countries). All terms are compliant with the Glossary of the WHO CC for Pharmaceutical Pricing and Reimbursement Policies of the GÖG / Austrian National Public Health Institute (https://ppri.goeg.at/about_translations). Table 1    Abbreviations: HIC=high income countries, INJ=injectable, LMIC= lower-middle income countries, POW=Powder for Injection; TAB=tablets, UMIC=upper-middle income countries Decimals are rounded * Price available in only one country # Prednisolone § Mean (only two values available) Currency exchange rates as of April 12, 2022     ABBREVIATIONS BUP=Brand Unit Price; CPY=cost per-patient-per-year; INJ=injectable; NPP=Non-Proprietary Name Unit Price; POW=powder for injection; TAB=tablet ASSUMED DMT DOSAGE · Alemtuzumab: one 12mg vial/day i.v. in 5 consecutive days per year = 5 12mg vials per year · Azathioprine: (average dose) one 50mg tablet x 3/day (target dose 2.5mg/Kg/day) = 1,095 50mg tablets/year · Cladribine: one 10mg tablet/day for two weeks (2 one-week cycles); 1.75mg/Kg = twelve 10mg tablets per cycle (weight range 60 to 70kg) · Cyclophosphamide: 750mg/square meter (900mg)/4 weeks i.v. = 13 vials per year · Dimethylfumarate: one 240mg tablet bid = 730 240mg tab per year · Fingolimod: one 0.5mg cap/day = 365 0.5mg caps per year · Glatiramer acetate: one 40mg vial x 3/week s.c. = 156 40mg vials per year · Interferon beta 1a (Avonex ®): one 0.03mg vial/week i.m. = 52 0.03mg vials per year · Interferon beta 1a (Rebif ®): one 0.22mg - 0.044 mg vial x 3/week s.c. = 156 0.22 mg vials per year · Interferon beta 1b: one 0.250 mg vial every other day s.c. = 182 0.250 mg vials per year · IvIG: 1,000mg/Kg/4 weeks (60Kg) i.v. = 60g/4 weeks i.v.= 780g/year (dosage as in Hommes 2004) · Methotrexate: 7.5mg (3 2.5mg tablets)/week = 156 tablets per year · Methylprednisolone: 1,000mg vial/4 weeks i.v. = 13 1,000mg vials per year · Mitoxantrone: 8 mg/square meter/month i.v. =12 2mg/ml vials 10 ml per year · Natalizumab: one 300mg vial/4 weeks i.v. = 13 300mg vials per year · Ocrelizumab: 600mg/6 months i.v.= four 300mg vials per year · Ofatumumab: one 20mg vial/month s.c.= twelve 20mg vials per year · Ozanimod: one 0.92 mg cap/day = 365 0.92mg caps per year · Peg-Interferon beta 1a: one 125mcg vial/2 week s.c. or i.m.= 26 125mcg vials per year · Ponesimod: one 20mg tablet/day (maintenance dose) = 365 20mg tablets per year · Rituximab: four 500mg vials i.v. in one session per year (starting dose 1,000mg i.v. twice two weeks apart; retreatment 1,000mg (two vials) i.v. after 6-9 months · Siponimod: one 2mg tablet/day = 365 2mg tablets per year · Teriflunomide: one 14mg tablet/day = 365 14mg tablets per year  ABBREVIATIONS CAP=capsule; POW=powder for injection; TAB=tablet | Affordability of the different DMTs is a complex topic as drug prices are not always publicly available or transparent. Pathways to affordability: We are aware that tiered pricing has been used in some countries, where substantially lower prices can be negotiated for specific countries or health systems relative to income levels. For example, we are aware of a LMIC with 10 on-label DMTs fully reimbursed by their national health system. The price reductions from listed prices can be at least as high as 75%. If a MS medicine is listed on WHO or national EML, a number of avenues to tackle availability and affordability of MS medicines can start through working with our key stakeholders. We can also further develop our relationships with other international organisations such as: 1. The Clinton Health Access lnitiative, who are willing to work with the WHO to improve drug access and delivery by resolving the various barriers that are impeding progress. 2. The Medicines Patent Pool is interested to work closely with us to identify opportunities to use voluntary licensing for any patented small molecules for MS, particularly if they are added to the WHO EML. MSIF has also created a theoretical framework for pooled price negotiations for the African region, which would need to be triggered by the listing of DMTs onto the WHO EML. Panel discussion: Drug cost is the major driver of resource requirements, but the panel identified the following additional resource requirements: lab-based diagnostics/monitoring (e.g. JCV testing for natalizumab and and complex monitoring for fingolimod), pre-screening and vaccinations (not implemented everywhere yet, but recommended for natalizumab, ocrelizumab, rituximab, fingolimod, siponimod), costs related to storage (e.g continuous electricity supply to maintain cold chain for GA, IFNs, natalizumab, ocrelizumab, rituximab, siponimod), management and disposal, pre-infusion preparation and human resources for administration (infusion: natalizumab, ocrelizumab, rituximab) and travel costs by patients to clinics and associated costs for medication to manage side effects. JCV testing needed in particular for natalizumab was considered a considerable issue, although this was sometimes covered by the pharmaceutical company and may be more relevant for feasibility. S1P receptor modulators (fingolimod, siponimod) require dermatology screening and opthalmology, otherwise age-appropriate cancer screening with all DMTs. Panel set the following thresholds compared to placebo, from a global perspective with focus on LMICs. They were based on medium/minimum wage and health care expenditure in LMICs. Large costs: >$1000/year/patient Moderate costs: >$100/year/patient Negligible costs/cost-savings: less than $100 Large: >$1000/year/patient: interferon beta 1a, interferon beta 1b, natalizumab, fingolimod, siponimod, glatiramer acetate, rituximab, ocrelizumab Moderate costs: azathioprine Negligible/cost-savings: methotrexate To make the final judgements on resource requirements, the panel considered whether the additional considerations would change the judgements. It was concluded that they would only add more cost onto the 'large' costs, so the judgments remained the same. It was noted that not all DMTs in the large cost category were the same. Rituximab was highlighted as the costs are generally lower, and significantly lower when compared against ocrelizumab, which has a similar mode of action. In UMIC median price: rituximab is 89% less than ocrelizumab. Rituximab is also already listed on the WHO EML and used (e.g. feasible, affordable, available) in many countries for a number of other conditions. The panel noted immunoglobulins are very high cost, even by comparison with other medicines. | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Certainty of evidence of required resourcesWhat is the certainty of the evidence of resource requirements (costs)? | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Judgement | Research evidence | Additional considerations | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Cost effectivenessWhich intervention does the cost effectiveness favor? | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Judgement | Research evidence | Additional considerations | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Cost-effectiveness is influenced by resource requirements, which are influenced by the medicines patent status. Patent landscape of DMTs available here: http://www.msif.org/wp-content/uploads/2022/03/DMTs-patent-overview-March-22.pdf We performed a systematic review of economic studies on each available DMT in the treatment of PMS when compared to another active DMT or to no DMT (plus best supportive care), from a payer as well as from a societal perspective. All types of economic analysis were consiedered: budget impact analysis, cost-effectiveness analysis (CEA), cost-utility analysis (CUA) and cost-benefit analysis (CBA) conducted in model-based or trial-based frameworks. Searches adopting filters specific to economic evidence were performed on February 17, 2022, on the following databases: MEDLINE, EMBASE and SCOPUS. The search retrieved 5,235 references from which 15 economic analysis studies were selected as eligible. Full text assessment brought to include in our analysis 7 studies (Forbes 1999, Kobelt 2000, Kobelt 2003, Prosser 2004, Zimmermann 2018, Bolanos-Diaz 2019, Schur 2021). All were performed in HICs except one (Bolanos-Diaz 2019) that was developed in Peru, an UMIC. Four were cost-effectiveness modelling studies, three were cost-utility analyses. Four of them were foscussed on people with SPMS (Forbes, 1999, Kobelt 2000, Prosser 2004, Schur 2021) while the remaining included people with CIS, RRMS, SPMS or PPMS, but presented separate data for progressive forms. All but one (Forbes 1999) cost-effectiveness analyses were based on Markov models for disease progression over variable duration on progression; health state related to disability was evaluated by means of the EDSS score. The effectiveness component of the model was based on evidence from RCTs or systematic reviews and - for long-term evaluation - from large cohort studies on the natural course of MS. The time horizon went from 30 months to lifetime. In several analyses, the most sensitive variables of the model were treatment adherence and direct cost of drugs. Notes Health effects are usually measured as life-years gained (LYGs) or quality-adjusted life-years (QALYs), accounting also for quality-of-life outcomes. Cost-effectiveness analysis (CEA) is usually performed by means of LYGs, and the parameter of interest is the incremental cost-effectiveness ratio (ICER). In cost-utility analysis (CUA) QALYs are commonly used and the parameter of interest is called incremental cost-utility ratio (ICUR). The terms ICER and ICUR are sometimes not distinguished and whether the result is expressed in LYGs or QALYs depends on the context. The ICER or ICUR is compared with the (official or approximate) willingness to pay for each unit of effect (LYG or QALY) gained. The per-QALY gained willingness-to-pay threshold is usually based on per capita Gross Domestic Product (GDP). For developing countries WHO recommends a threshold 1 to 3 times the GDP (Bertram 2016, doi: 10.2471/BLT.15.164418) . Direct costs are usually referred to cost of drug, its acquisition, administration, monitoring, natural disease management, relapse treatment, and adverse event management. Indirect costs are usually referred to loss of productivity, absenteeism, early retirement, travelling cost to reach healthcare facilities. Intepretation Conclusions were variable: in older studies (Forbes 1999, Kobelt 2000) when IFN was the main available treatment in clinical practice, its cost-effectiveness was considered either poor (Forbes 1999) or acceptable, depending on the assumed threshold of willingness to pay for an additional QALY gained. More recent studies showed a favourable cost-effectiveness of IFN beta products (Kobelt 2003) particulary if combined with tailored patient support programmes (Bolanos-Diaz 2019). Economic analysis in the US from a payer's perspective found an unfavourable cost-effectiveness for IFN beta and glatiramer acetate in people with SPMS (Prosser 2004) and for ocrelizumab in PPMS (Zimmermann 2018). Siponimod was found to be cost-effective in a recent Swiss study in adults with active SPMS (Schur 2021). The main limitation of DMTs in SPMS and PPMS is their relatively modest effect combined with a disproportionately high price, making them cost-effective only if assuming a high threshold of willingness to pay for QALY gain. The evidence base for the effectiveness and cost-effectiveness of DMTs in RRMS and SPMS is poor. The clinical effectiveness and cost-effectiveness of alternative sequences of DMTs is uncertain. Uncertainty in the cost-effectiveness estimates of DMTs raises mainly from: - the relatively short follow up of trials and the scarcity of evidence on long term effectiveness of DMDs - the lack of economic analyses in countries other than HICs. Economic analysis studies on DMTs for PMS  | Evidence on cost-effectiveness was only found for interferon, GA, ocrelizumab and siponimod. The studies on siponimod (Schur 2021) and interferon from Peru (Bolanos-Diaz 2019) have risk of bias, as they were conducted by the pharmaceutical company or authors were employed by the company. A Norwegian HTA study from 2021 referenced similar effectiveness of rituximab to ocrelizumab and fingolimod, but at a multitude lower price. No modelling was done. However, as the Norwegian HTA study was not formally included in the evidence review, it received the judgement "no included studies". The panel noted issues with inconsistency, variability and poor evidence-base. Generally, cost-effectiveness found to be poor or acceptable for interferon, GA and ocrelizumab. The only positive finding was for siponimod with active SPMS. Main issues: (1) High price of DMTs, so cost-effectiveness only positive if willingness to pay was high for QALY gained. (2) Effectiveness is based on short-term RCTs, so it is unknown what the long-term effectiveness of these drugs are. (3) Most studies are from HICs. (4) Some studies are 20 years old, so need to be interpreted with caution. The panel noted that cost-effectiveness for Interferon beta 1a and 1b has improved over time, potentially due to follow-on products becoming available and reduction in price. The only study in an UMIC, Peru, found interferon combined with the personalized support programs for patients cost effective for pwPMS. The HTA process often has more to do with price negotiations than objective cost-effectiveness. The huge cost of disability is generally longer term. Whether DMTs prevent long term disability is a question that will be answered in 5-10 years. The real value is seen when looking across the lifespan and you can account for the cumulative effect. There are some studies showing substantial effect on slowing disability worsening of platform inectable therapies and all pooled DMTs in RRMS: Palace J, Duddy M, Lawton M, et al. Assessing the long-term effectiveness of interferon-beta and glatiramer acetate in multiple sclerosis: final 10-year results from the UK multiple sclerosis risk-sharing scheme. J Neurol Neurosurg Psychiatry 2019;90:251-260. Kalincik T, Diouf I, Sharmin S, et al. Effect of Disease-Modifying Therapy on Disability in Relapsing-Remitting Multiple Sclerosis Over 15 Years. Neurology 2021;96:e783-e797. The panel noted that the lack of studies is a real potential confounder in our interpretations of true cost effectiveness. For example, the fact that Kaiser in the US and Sweden prefer to use rituximab may speak to the real cost effectiveness of the medication, regardless of the available studies/evidence. It was suggested that the evidence-base was not meeting baseline requirements to be used for making judgements globally and the cost-effectiveness of ocrelizumab, interferons, GA and siponimod were all judged to 'vary'. Panel members present with no COI voting (10): 1 Probably favours comparison i.e. no DMT 8 Varies in different situations/settings/countries 1 Abstain | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
EquityIf recommended, which intervention would reduce health inequities the most? | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Judgement | Research evidence | Additional considerations | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
We included in this synthesis 2 systematic reviews (Onuorah 2022, Roddam 2019), one survey (Carnero Contentti 2021), two retrospective studies (Gomez-Figueroa 2021, Hartung 2020) and one register-based study (Khayambashi 2020) reporting results on equity. Furthermore we consider results from 6 studies suggested by panel members. POPULATION-LEVEL -Access to DMTs in disadvantaged groups Race Onuorah et al., 2022 performed a systematic review of RCTs to assess the representation of minority patients in DMTs trials. Among 44 phase 3 trials reviewed, 37.8% did not report race, 31,1% reported race as proportion of white participants only, and only 31.1% reported detailed information on race. In the selected studies with information on racial and ethnic representation, the median percentage of White participants was 93.8% (range 78.5–99.6% across 28 studies), 1.9% for Black participants (range 0.1–8.1% across 14 studies), and 0.5% for Asian participants (range 0.1–14.5% across 11 studies). No patient- or health care provider -facing DMT websites reported data on race and ethnicity in pivotal trials. These findings are consistent with the hypothesis that ethnic minority populations are consistently underrepresented in clinical trials of MS, leading to limited data on the effectiveness of treatments in these groups of patients and lack of an evidence-based approach to treatment. Additional evidence suggested by panel members that confirm the above results: Avasarala 2014: Evidence highlight that as compared with white Americans; African Americans are thought to have a lower risk for developing MS but a greater risk of disability. Compared with white Americans with MS, African Americans with MS have a more aggressive disease course and a greater risk of early second relapse. Hence, differences in MS susceptibility, disability outcomes, and clinical course may have biologic origins related to race/ethnicity. Nevertheless, the most important clinical trials on drug treatment for MS show that the percentage of white American patients was prevalent while other races/ethnicities have been little investigated, for that it is difficult to categorize treatment options for African American patients due the different characteristics of the disease in this population. The study notes also that African American patients probably seek help at referral centers only after severe disability ensues, which introduces selection bias. Avasarala 2019: The study reports lack of recruitment of non-White patients with MS in clinical trials with no data compared how drugs performs in African American versus White American. MS drugs approved by the FDA do not contain efficacy data for minorities and therefore clinicians are unable to discuss the efficacy data of any MS drug with their non-White patients. The lack of any drug data in non-White patients with MS in published clinical trials is troublesome. The authors state that reporting baseline patient demographic data characteristics in the published literature must be made mandatory. Avasarala 2021: The study confirms what already seen in the previous ones (Avasaral 2014 and 2019) and conclude that the disease characteristics and phenotype of MS among Blacks and Hispanics are typically aggressive and for this reason alone, if not for any other metric, there needs to a radical shift in allotment of funds devoted to promoting drug research in minority population Below a table summarizes the results.  Liu 2020: Lack of reported race and enrollment among Blacks in clinical studies considering the efficacy of Siponimod for MS Socio-economic status Roddam et al., 2019 performed a systematic review investigating differences in access to prevention services, healthcare services, treatments and social care between inequality groups. They found evidence of inequalities in access to services with a trend for worse access among men, older age groups, those from lower socio-economic groups, the least educated, non-Whites, those with mental health problems and those from rural areas. In the studies on access to DMTs, older age and lower socioeconomic status were consistently associated with a lower rate of uptake, while race and sex were not. Carnero Contentti et al. 2021 conducted a web-survey in Argentina to investigate the barriers and utilization of MS care services in Latin America. They found that between 65.7% (Uruguay) and 95.8% (Paraguay) of patients with MS in the region reported DMT treatment prescribed immediately after MS diagnosis. Between 2.8% and 21.9% reported having problems obtaining medications because these were not covered by their insurance plan. Nevertheless, over 80% (except for Ecuador (64%) and Honduras (60%)) indicated taking DMT as prescribed by their clinicians during the last year. Examining DMT use in greater detail, they found significant level of innovator DMT replacement by generic or biosimilar compounds in Argentina (68%) and much less in Chile, Colombia, Honduras, and Mexico. Lack of health insurance and longer duration of MS were associated with inadequate treatment, while higher level of education and retaining employment improved treatment delivery. Lack of health insurance was associated with problems obtaining DMT whereas having a high level of education made access to DMT easier (first prescription or follow- up medication). Gomez-Figueroa 2021 reported the results of retrospective study conducted in Mexico. The study includes a mixed population (84.5% RRMS, 11.6% SPMS, 3.9% PMS). When comparing the lower versus higher level of socio-economic status (SES), a significant association was found on the percentage of patients with a higher level of disability (EDSS >6) at arrival. A greater proportion of patients with very low SES did not have access to a DMT compared to people with a higher level SES. Conversely, patients with high SES had more access to high efficacy therapies compared to lower level of SES (35.7% vs 14.8%, p<0.001). Lower SES had an association with the proportion of patients not receiving any DMT, and a higher proportion of SPMS. Hartung 2020: retrospectively compared patterns of DMT initiation for MS among all U.S. Medicare beneficiaries with and without low income subsidy (LIS) benefits. The time until DMT initiation was significantly lower in those with LIS benefits relative to those without. Of those who initiated, the full LIS recipients initiated on average 22 days sooner than non-full LIS recipients (114.9 days ± 95.8 days vs 137.0 days ± 106.6 days, p<0.0001). Even after adjustment for a broad spectrum of possible demographic and co-morbid condition confounders, those receiving LIS benefits remained 40% more likely to initiate a DMT. The effect of reduced cost-sharing on DMT initiation was consistent across a variety of demographic subgroups. Sex Khayambashi 2020: evaluated health care utilization in transgender and non-heterosexual persons with MS using data from the North American Research Committee on Multiple Sclerosis (NARCOMS) Registry. Outcomes of interest were any emergency room visits (ER) in the prior six months; (ii) any hospital admissions in the prior six months; and (iii) any DMT use in the prior six months. The frequency of any ER visits, any hospital admissions, and DMT use did not differ according to gender identity and sexual orientation. This finding should be interpreted cautiously given the small number of transgender participants, and the short, 6-month reference study period. GLOBAL PERSPECTIVE - Cost Laurson-Doube 2020: Access to treatment and treatment choice are dictated by available resources, and resource allocation in many world regions is influenced by the WHO EML. Resource-poor regions cannot afford highly priced therapeutics and available guidelines do not consider regional safety and efficacy issues that are likely to differ markedly from those in resource-rich countries. Editorial highlights the necessity of guidelines for MS management in low-resource environments in which evidence should be integrated into proposals for sustainable improvement of care. Calculations of cost-effectiveness from high-income areas are often meaningless to low-resource areas where the financial burden of a disease is unknown. Laurson-Doube 2021 reported data on the use of off-label DMTs: a total of 89 countries (87%) use at least one off-label DMT to treat MS. The authors discussed the difference between availability and affordability of off-label vs on-label MS DMTs in HICs compared to LMICs, UMICs and LICs. An ethical use of off-label DMTs should be provided if: a) on-label DMTs are not tolerated, unsuitable for the best clinical outcome, unavailable or unaffordable; b) evidence of efficacy and safety on off-label DMTs is available; c) information on balance between health benefits and risks by health care professionals is available; d) clinical outcomes and adverse events when using off-label DMTs is monitored. The development of guidelines and recommendations, evidence-based and following a structured and transparent approach, are crucial for supporting the standardisation and improvement of care, and to inform policy and reimbursement decisions for the use of off-label DMTs. -Availability Atlas of MS clinical management 2021. A global survey on the availability of resources and services for people with MS in different regions of the world found a widening gap between HICs and LICs in the access to DMTs. They found that: -14% of countries surveyed report having no licensed DMTs available for pwMS. In the African region this figure is 60%, and 70% of LICs report no access to licensed DMTs; -the use of off-label DMTs is common, reported by experts in 87% of countries worldwide. Lack of availability of similar licensed DMTs in the country or unaffordability of licensed DMTs are some of factors that can drive off-label DMT use; -globally, 11% of countries do not use moderate efficacy licensed DMTs, and 20% of countries do not use good efficacy licensed DMTs. In particular, 25% of countries report that they do not use high efficacy licensed DMTs. This strongly correlates with income, with 50% of LMICs and 100% of LICs not using high efficacy DMTs. Among barriers to DMT administration they identified: -the cost to the government, healthcare system or insurance provider; - concern about the side effects by people with MS -lack of healthcare professionals and a lack of knowledge of DMTs amongst professionals -bureaucracy, inefficiency or complexity within the healthcare system Lekha Pandit 2021: For chronic disorders such as multiple sclerosis (MS), personal funding of therapy is a strain on poor family resources and limits access to care, particularly for the uninsured majority living in countries with deficient national health care programs. In such situations, treatment needs of pwMS in LMICs need to be addressed pragmatically. The MSIF’s recent Atlas of MS survey showed that 87% of countries use at least one off-label therapy to treat MS. Access to therapy was restricted in the majority of countries surveyed with 70% of LICs having no on-label MS DMTs. Mandating the requirement of phase 3 trials or head to-head comparator studies before accepting an affordable off-label drug (repositioned generic or bio similar) as standard for MS therapy is impractical. Treatment guidelines should look beyond therapies advocated in high-resource settings and rely on availability and affordability of other safe alternatives. -Mode of administration, frequency of administration, storage No evidence was found. Below a summary of evidence retrived following PROGRESS framework:  KEY POINTS · Several studies have explored the access to DMTs in disadvantaged groups · Under-representation of ethnic minority populations in clinical trials leading to limited data on the effectiveness of treatments in these groups; · Inequalities in access to services with a trend for worse access among men, older age groups, those from lower SES groups, the least educated, non-Caucasians, those with mental health problems and those from rural areas; · Lack of health insurance and longer duration of MS were associated with inadequate treatment, while higher level of education and retaining employment improved treatment delivery. · Lack of health insurance was associated also with problems obtaining DMT whereas having a high level of education made access to DMT easier · A greater proportion of patients with very low SES did not have access to a DMT compared to people with higher SES level · The frequency of any ER visits, any hospital admissions, and DMT use did not differ according to gender identity and sexual orientation · In theUS Medicare beneficiaries with and without LIS benefits have different access to a DMT · Cost and availability of DMTs are barriers both at the population-level and at the global-level References - Onuorah Helen-Margaret, Ethan Meltzer, Amanda Montague, Alexis Crispino, Avery Largent, Ashlea Lucas, Leorah Freeman. Enrollment of Non-White Participants and Reporting of Race and Ethnicity in Phase III Trials of Multiple Sclerosis DMTs: A Systematic Review. Neurology 2022 Jan 19;10.1212/WNL.0000000000013230. doi: 10.1212/WNL.0000000000013230. - Roddam H et al. Inequalities in access to health and social care among adults with multiple sclerosis: A scoping review of the literature. Multiple Sclerosis and Related Disorders 2019;28: 290-304. - Carnero Contentti E, Giachello S, Correale J. Barriers to access and utilization of multiple sclerosis care services in a large cohort of Latin American patients. Multiple sclerosis (Houndmills, Basingstoke, England). 2021;27(1):117-29. -Gomez-Figueroa E, de Sarachaga AJ, Garcia-Estrada C, Casallas-Vanegas A, Delgado-Garcia G, Garcia-Martinez P, et al. Socioeconomic status and access to multiple sclerosis treatment in Mexico. Multiple sclerosis and related disorders. 2021;52:102967. -Khayambashi S, Salter A, Tyry T, Cutter GR, Fox RJ, Marrie RA. Gender identity and sexual orientation affect health care satisfaction, but not utilization, in persons with Multiple Sclerosis. Mult Scler Relat Disord. 2020 Jan;37:101440 - Hartung DM, Johnston KA, McGregor JC, Bourdette DN. The effect of out-of-pocket costs on initiation of disease-modifying therapies among medicare beneficiaries with multiple sclerosis. Mult Scler Relat Disord. 2020(2211-0356 (Electronic)). - Avasarala J. Inadequacy of Clinical Trial Designs and Data to Control for the Confounding Impact of Race/Ethnicity in Response to Treatment in Multiple Sclerosis JAMA Neurol 2014 Aug;71(8):943-4. doi: 10.1001/jamaneurol.2014.79. - Avasarala J. FDA-approved drugs for multiple sclerosis have no efficacy or disability data in non-Caucasian patients. CNS Spectr 2019 Jun;24(3):279-280. doi: 10.1017/S1092852918001517. -Avasarala J., Phenu Zachariah, Breck Turner. Pivotal clinical trial enrollment of Blacks in multiple sclerosis or neuromyelitis spectrum disorder: when will we achieve parity? CNS Spectr 2021 Feb 10;1-3. doi: 10.1017/S1092852921000183. - Liu M, Aniwaa Owusu Obeng. Siponimod and CYP2C9 Allele Prevalence Among Blacks. J Clin Pharmacol 2020 Apr;60(4):429-431.doi: 10.1002/jcph.1546. - Laurson-Doube J, Rijke N, Costello K, McDonell J, Giovannoni G, Banwell B et al. Health-care disparities for people with multiple sclerosis. The Lancet Neurology 2020;19(3):207-208 - Laurson-Doube J, Nick Rijke, Anne Helme, Peer Baneke, Brenda Banwell, Shanthi Viswanathan, Bernhard Hemmer, Bassem Yamout.. Ethical use of off-label disease-modifying therapies for multiple sclerosis. Mult Scler 2021 Aug;27(9):1403-1410. doi: 10.1177/13524585211030207 - Lekha Pandit . Fair and equitable treatment for multiple sclerosis in resource-poor regions: The need for off-label therapies and regional treatment guidelines. Mult Scler 2021 Aug;27(9):1320-1322. doi: 10.1177/13524585211028806. - The Multiple Sclerosis International Federation – Atlas of MS – 3rd Edition, part 2: clinical management of multiple sclerosis around the world (April 2021). Available at: Atlas-3rd-Edition-clinical-management-report-EN-5-5-21.pdf (msif.org) Protocol: https://osf.io/5edjf | The panel noted the lack of evidence considering the equity issues between the specific DMTs. Atlas of MS shows unequal access to DMTs between LMICs and HICs. 'High efficacy' DMTs (natalizumab, ocrelizumab, alemtuzumab) are even less available. The panel noted the following factors affecting equity: cost/income, route of administration, access to healthcare facilities, storage, e.g. cold-chain requirements. Important to consider actual care delivery. For many patients who are poor/unhoused/have other barriers to adherence, a twice-year infusion is often preferable and easier, even if there are considerable costs to getting to an infusion centre, to a self-injectable that they may have to carry with them and keep refrigerated (yet away from children). Important to note when we rate the relative impact of equity of self-injectables vs infusions. The panel discussed the difference between health equity vs financial equity. Health equity would increase more if a moderate cost but higher efficacy DMT was available than if a very inexpesnive but less effective DMT was recommended. Health equity considerations if not treated include direct costs of disability progression, unemployment, caring responsibilities for family, equipment and living arrangement modifications, not only cost of medicine. Cost of medicine is also potentially modifiable. This guideline’s primary purpose is to help inform an application to the WHO EML, which is meant to impact availability and costs for medicines that are efficacious. Other considerations relevant for equity: 1. Access to electricity and refrigeration (maintain cold-chain and storage) and access to healthcare facilities (to access infusion suites). These considerations would seem to favour oral treatments. 2. Pregnancy and breastfeeding, as disease onset is normally at this stage and women 2-3x more affected than men. GA, interferons can be used, rituximab, ocrelizumab and natalizumab can be used with careful timing of the dosing. Azathioprine can potentially be used with very careful dosing. Fingolimod, siponimod and methotrexate have specific contraindications due to risk to the foetus and cannot be used during pregnancy. Azathioprine, although a category D medication, can be used if the benefits outweigh the risks. It is sometimes used in NMOSD. Azathioprine crosses the placenta, but the foetal liver lacks the enzyme inosinate pyrophosphorylase, which converts azathioprine to its active metabolite, 6-mercaptopurine; thus, the foetus is protected from the agent's teratogenic effects. A meta-analysis of four studies that evaluated azathioprine/6-mercaptopurine use in 312 pregnant women with inflammatory bowel disease (IBD) found no increased risk for spontaneous abortion, prematurity or low birth weight. However, an increased risk for congenital abnormalities was found in women taking the drug, compared with women with IBD not on medications (OR, 2.95; 95% CI, 1.03-8.43). Panel judgements: Fingolimod, ocrelizumab, siponimod, natalizumab would probably reduce equity due to required pre-tests, monitoring and mode of administration logistics and costs. The availability and cost of treatment were also considered. Glatiramer acetate, interferon beta 1a (Avonex Rebif), interferon beta 1b, methotrexate were judged as 'probably no impact' due to better availability, less pre-tests and monitoring requirements. The cold-storage and frequent injections were noted as barriers for interferon and GA. The panel judged that azathioprine, rituximab 'probably increase' equity as they are already listed on the WHO EML (but not with MS indication) and many national EMLs, increasing availability and feasibility. Their low price was also noted. The panel judged immunoglobulin as 'reduce' due to very high cost, poor access, difficulty in sourcing, storage and cold-chain required. | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
AcceptabilityWhich intervention is more acceptable to key stakeholders? | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Judgement | Research evidence | Additional considerations | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Consideration for people affected by MS -Dropouts due to any cause from the NMA is a proxy for acceptability.
-Mode and frequency of administration Mardan 2021: Performed a systematic review to measure adherence and discontinuation rates of oral and injectable DMTs using: medication possession ratio (MPR); proportion of days covered (PDC); binary adherence cut-off score, reported at least 80% adherence unless otherwise specified, or effect size and standard error. Among 61 observational studies adherence varies across studies and is suboptimal. When compared with injectable DMTs and measured using mean adherence a significant improvement in 12-month medication adherence for oral DMTs was found. The improvement contrasted with a 12-month oral and injectable adherence using a cut-off score of at least 80% to determine adherence, which showed no significant difference. Furthermore, there was no appreciable difference in 12-month discontinuation rates between oral and injectable DMTs. Nicholas 2020: The review aims to conduct a systematic literature review to assess the availability and variability of oral DMD adherence and/or persistence rates for once- and twice-daily oral DMDs in patients with MS using real-world data. Adherence was measured differently across studies. Approximately one in five patients with MS do not adhere to, and one in four discontinue, daily oral DMT before 1 year. No differences between US- and no-US-based studies and between Black patients and Hispanic and Latinx patients. Perez 2021: retrospective review of electronic medical records considering a multi-ethnic cohort of MS patients; data showed a differential response to therapeutic intervention by race and ethnicity in terms of tolerability profiles: Blacks had poor tolerability to first-line treatment with interferons respect to Hispanics and Whites. While white patients tolerated glatiramer acetate less frequently, teriflunomide, fumarates, S1P inhibitors and the monoclonal antibodies were relatively well tolerated across ethnic groups, with a less than 20% discontinuation rate due to adverse events. Alhazzani 2019: cross-sectional study; found more adherence with higher levels of education (i.e., secondary or university than lower educational levels (i.e., illiterate, primary, or intermediate levels), highest adherence in patients with oral treatment (fingolimod capsules), followed by beta interferons which is injected intramuscularly, as well as interferon beta-1b and interferon beta-1a, which are injected subcutaneously. No difference in adherence based on other characteristics (i.e., age, gender, region, marital status, age at disease onset, duration of disease, number of hospital admissions, number of attacks within the last 2 years, duration of used medications in years, or disease severity. -Satisfaction with the treatment regimen Ting 2015: conducted a systematic review of clinical studies that reported MS patient satisfaction with their disease-modifying therapies (DMTs) using the Treatment Satisfaction Questionnaire for Medication (TSQM) (score range 0-100). The DMTs studied included interferon beta-1b, glatiramer acetate, fingolimod, teriflunomide, and natalizumab. TSQM assesses four key dimensions of treatment satisfaction: Effectiveness; Side Effects; Convenience; and Global Satisfaction. Change from baseline (CFB) at 6 months on the effectiveness subscale ranged from 1.8 to 26.9, convenience subscale from 3.6 to 41.2, and global satisfaction subscale from 2.9 to 20.4. CFB at 6 months was generally higher for natalizumab and fingolimod compared with injectable platform DMTs, although this finding may be confounded by the differences in study design and patient characteristics. Eagle 2017: prospective observational cohort study, examined treatment satisfaction (effectiveness, side effects, convenience and overall satisfaction) in MS with TSQM by comparing patients’ satisfaction with oral, injectable and infusion therapies. The three injectable treatments were interferon beta-1a intramuscular (IFNβ 1a IM), interferon beta-1a subcutaneous (IFNβ 1a SC), and glatiramer acetate (GA). The infusion treatment was natalizumab (NTZ). The oral treatments were fingolimod (FTY) and dimethyl fumarate (DMF). The most consistent differences among the groups were related to the convenience of the medication, with oral medications have the highest scores and infusion medications the second highest. In terms of side effects, significant differences between all groups in terms of the presence of side effects were found, with the infusion medication having the lowest rate of side effects and the injectable medications having the highest. At the same time, the side effects of the injectable medications had a significantly smaller effect on mental function than the other two treatment groups among the subjects who had side effects. In terms of overall satisfaction subscale, the oral medication group reported significantly higher satisfaction compared to the injectable group in the total score, and the same relationship was seen in the question related to satisfaction with the medication. Table 2 reports the treatment satisfaction outcomes compared across the treatment groups for the routes of administration (From Eagle 2017)  Fragoso 2016: survey that assessed the degree of satisfaction of patients with MS regarding treatments with DMTs prescribed at five different Brazilian MS Units. Questions related to personal impressions of treatment benefits, tolerability, convenience of use and general satisfaction with the treatment was assessed by individual interview. For all DMTs, over 80% of the patients perceived that they were beneficial. The convenience of oral drugs was higher than that of injectable medications, but the difference was less than 10%. Tolerability was the aspect scoring lesser values, ranging from 40 to 50% for all treatments. Morillo Verdugo 2019: cross-sectional study; Patient satisfaction for the type of administration was higher with oral route than with injectable treatment but no differences in adherence based on the administration route (oral [63%] vs injectable [77%]. Among oral treatments, the highest non-compliance rate appeared in patients receiving dimethyl fumarate (65%), followed by fingolimod (29%) and teriflunomide (7%). Among injectable drugs, the highest non-compliance rate was observed in patients who were treated with interferon beta-1b (47%), followed by interferon beta-1a (30%) and glatiramer acetate (26%). Older age, more treatments received, time to diagnosis 5–10 years, better cognitive and memory status, being married/in a union, having received clear information about the treatment and higher satisfaction with the current administration route are associated to treatment adherence. -Type of side effects Atlas of MS clinical management 2021. A global survey on the availability of resources and services for people with MS in different regions of the world reported that the second most common barrier in access DMTs, reported by experts from 41 participating countries (39%), is that people with MS do not take DMTs when offered them, often due to expense or concern about the side effects. -Requirement to attend a healthcare facility for administration and/or follow up monitoring No evidence was identified Considerations for clinicians No evidence was identified that considered acceptability from a clinician’s perspective Considerations for payers No evidence was identified that considered acceptability from a payers perspective Considerations for health systems No evidence was identified that considered acceptability from a health system perspective KEY POINTS · In comparison with placebo, results are in favour of placebo for: Rituximab (very low certainty of evidence); Interferon beta 1a (high certainty of evidence); Glatiramer acetate (high certainty of evidence); Immunoglobulins (very low certainty of evidence). Results are in favour of drugs for: Azathioprine (low certainty of evidence); Interferon beta 1b (high certainty of evidence); Metrotrexate (very low certainty of evidence); Siponimod, Natalizumab, Fingolimod, Ocrelizumab (for all high certainty of evidence). · At 12 months one review showed better results for oral DMTs compared with injectable DMTs; another one found that approximately one in five patients with MS do not adhere to, and one in four discontinue, daily oral DMT before 1 year. · Blacks had poor tolerability to first-line treatment with interferons respect to Hispanics and Whites. While white patients tolerated glatiramer acetate less frequently, teriflunomide, fumarates, S1P inhibitors and the monoclonal antibodies were relatively well tolerated across ethnic groups, with a less than 20% discontinuation rate due to adverse events. · Association was found between adherence to DMTs and level of education: more adherence with higher levels of education, highest adherence in patients with oral treatment (fingolimod capsules), followed by beta interferons which is injected intramuscularly, as well as interferon beta-1b and interferon beta-1a, which are injected subcutaneously. No difference in adherence based on other characteristics. · Overall, results are in favour of oral DMTs, one study found at 6 months higher satisfaction for natalizumab and fingolimod compared with injectable platform DMTs, although says that this finding may be confounded by the differences in study design and patient characteristics. · no differences in adherence based on the administration route. Among oral treatments, the highest non-compliance rate appeared in patients receiving dimethyl fumarate, followed by fingolimod and teriflunomide. Among injectable drugs, the highest non-compliance rate was observed in patients treated with interferon beta-1b, followed by interferon beta-1a and glatiramer acetate. · Convenience in the use of oral medications is highest for oral DMT, followed by infusion medications. Otherwise, in terms of side effects, patients reported a lowest rate of side effects with infusion medication and an highest effect for the injectable medications References -Mardan J, Hussain MA, Allan M, Grech LB. Objective medication adherence and persistence in people with multiple sclerosis: A systematic review, meta-analysis, and meta-regression. Journal of Managed Care and Specialty Pharmacy 2021;27(9). - Nicholas JA et al. Real-world adherence to, and persistence with, once- And twice-daily oral disease-modifying drugs in patients with multiple sclerosis: A systematic review and meta-analysis. BMC Neurology 2020; 20(1): 281. -Pérez CA. Racial and ethnic disparities in treatment response and tolerability in multiple sclerosis: A comparative study. Multiple sclerosis and related disorders 2021;56 -Alhazzani A, Alqahtani M, Alahmarii M, Alamri N, Sarhan L, Alkhashrami S. Treatment satisfaction and adherence to medications among multiple sclerosis patients in Saudi Arabia. Egyptian Journal of Neurology, Psychiatry and Neurosurgery. 2019;55(1):57 - Ting J, Liu Y, Petrillo J, Sabatella G, Giannattasio G. Treatment satisfaction with disease modifying therapies in multiple sclerosis: A systematic review of studies using the treatment satisfaction questionnaire for medication (TSQM). Value in Health. 2015;18(7):A760-A1. - Eagle T, Stuart F, Chua AS, LaRussa A, Leclaire K, Cook SL, et al. Treatment satisfaction across injectable, infusion, and oral disease-modifying therapies for multiple sclerosis. Multiple sclerosis and related disorders. 2017;18:196-201. - Fragoso YD, Spessotto CV, Cavalli H, Sato HK, Eboni ACB, Goncalves MVM, et al. Patients' satisfaction with and views about treatment with disease-modifying drugs in multiple sclerosis. Arquivos de Neuro-Psiquiatria. 2016;74(8):617-20. -Morillo Verdugo R, Ramírez Herráiz E, Fernández-Del Olmo R, Roig Bonet M, Valdivia García M. Adherence to disease-modifying treatments in patients with multiple sclerosis in Spain. Patient Prefer Adherence. 2019 Feb 13;13:261-272. doi: 10.2147/PPA.S187983 Protocol: https://osf.io/5edjf | On-label/off-label status may be relevant to acceptability, e.g. clinicians being comfortable to prescribe off-label and pwMS making informed decisions. Key stakeholders to be considered include: patients, healthcare providers, policy makers/decision makers and payers. Acceptability by health systems is affected by resource requirements. MSIF has provided several pathways for affordability in criteria 7 'resource requirements'. Dropout due to any cause summary: In favour of no DMT: rituximab (very low certainty), interferon beta 1a (high certainty), GA (high certainty), immunoglobulins (very low certainty) In favour of treatment: azathioprine (low certainty), interferon beta 1b (high certainty), methotrexate (very low certainty), siponimod (high certainty), natalizumab (high certainty), fingolimod (high certainty), ocrelizumab (high certainty). The panel noted that the evidence needs to be interpreted with caution as there is an inherent bias linked to the availability of other DMTs, i.e. studies in 1990s would be less likely to have drop-outs than those in 2020 due the large number of other treatments available to switch to. The panel noted that evidence suggested oral treatments are more acceptable than infusion, which are both more acceptable than injectables. There are differences between preference and individuals may prefer less frequent infusion over daily oral medication. There is no clear link between drop-out data and mode of administration. The panel felt that if injectables (interferon and GA) were the only option available, pwMS would likely still feel they were acceptable for treatment. There may be issues with acceptability of GA in some world regions due to political issues, as originator was developed by an Israeli company. Cost may be relevant for acceptability to patients. If you can’t afford it, you cannot adhere to treatment. Difference in side-effects can influence acceptability and some of this may be linked with the drop-out data. Interferon or glatiramer acetate, infrequent skin changes 2-3 years after treatment starts. Interferon frequent flu-like symptoms. This should be based on expert opinion from the panel, as there is no systematic evidence. There have been some significant safety warnings introduced since regulatory approval, notably to natalizumab (PML risk with JCV) and fingolimod. The lack of capacity (e.g. MRI) or access to laboratory tests available (e.g. JCV testing) for required monitoring may be problematic, especially in some low-resouurce settings. JCV testing is sometimes provided by the pharmaceutical company, but this is not always the case and follow-on products are becoming available, where this service may not be implemented. A summary of EMA safety warnings can be found here: http://www.msif.org/wp-content/uploads/2022/08/EMA-safety-warnings_PMS_300522.docx [https://www.msif.org/supporting-documents-memp-etd/] Evidence shows risk of PML in JCV positive patients with natalizumab is extremely low during first 1-2 years of treatment (Ho PR, Koendgen H, Campbell N, Haddock B, Richman S, Chang I. Risk of natalizumab-associated progressive multifocal leukoencephalopathy in patients with multiple sclerosis: a retrospective analysis of data from four clinical studies. Lancet Neurol. 2017 Nov;16(11):925-933. doi: 10.1016/S1474-4422(17)30282-X. Epub 2017 Sep 29. PMID: 28969984.). Panel noted the catastrophic rebound risk if access is suddenly limited for natalizumab, fingolimod and siponimod. Pregnancy related safety issues should also be considered. Important to note, that in low-resource settings, any one DMT may be the only available option and people will still probably take it. For immunoglobulin, the panel judged as ‘probably no’ due to high cost, sourcing, storage and infusion requirements. All other DMTs were judged to be 'probably acceptable', with azathioprine and methotrexate 'acceptable' due to low cost, availability and oral mode of administration. | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
FeasibilityWhich intervention is more feasible to implement? | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Judgement | Research evidence | Additional considerations | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Long-term resource requirements and feasibility are influenced by the DMTs patent status around the world. Patent landscape of DMTs available here: http://www.msif.org/wp-content/uploads/2022/03/DMTs-patent-overview-March-22.pdf CONSIDERATION FOR PEOPLE AFFECTED BY MS -Cost Atlas of MS clinical management 2021. A global survey on the availability of resources and services for people with MS in different regions of the world found that it is common for people with MS to have to pay some or all of the cost of their DMTs, sometimes referred to as ‘out of pocket costs’. This was reported to occur in 60 countries (57%) worldwide, ranging from 39% of countries in Europe to 76% of countries in the Americas. The reasons people have to pay for DMTs are varied. Of the 60 country coordinators reporting that people have to pay at least some of their DMT costs: • 48% report the government, healthcare or insurance provider requires a co-payment or will only pay part of the cost • 40% report that people with MS do not have health insurance • 35% report that DMTs are not covered by health insurance • 35% report that even if people with MS have health insurance, the DMT recommended is not approved or they don’t meet the eligibility criteria. -Access to therapy Atlas of MS clinical management 2021 reported that even if people have access to DMTs, there are also barriers to the continuous provision of their treatment. Experts in almost half of countries worldwide report problems with the continuous provision of DMT treatment, meaning that once initiated on a DMT, people with MS are unable to receive future doses without interruption or delay. The main reasons cited are an irregular supply of DMT (27% of all countries) or the delays associated with people needing to get their reimbursement renewed (19%) or the need to take regular tests to prove continued eligibility (13%). -Off-label status Atlas of MS clinical management 2021. A global survey on the availability of resources and services for people with MS in different regions of the world found that the use of off-label DMTs (therapies that have not been approved specifically for MS) is common. Experts in 87% of countries report the use of off-label drugs to treat MS. It is common for people with MS to have to pay some or all of the cost of their DMTs, sometimes referred to as ‘out of pocket costs’. This was reported to occur in 60 countries (57%) worldwide, ranging from 39% of countries in Europe to 76% of countries in the Americas. -Mode of administration, frequency and storage of DMTs No evidence was found -Requirement to attend a healthcare facility for administration and/or follow-up monitoring No evidence was found CONSIDERATIONS FOR PAYERS -Cost Kotsopoulos 2020: The aim of this study was to estimate the effect of DMTs on government public economics by quantifying lost tax revenue and additional spending on social benefit transfer programs, i.e. transfers attributed to disability progression and preventable by DMTs, throughout a disease simulation model. The model simulates the natural history of cohorts of Swedish patients receiving no treatment (placebo) or one of the following DMTs: Interferon beta-1a, Pegylated interferon beta-1a, Dimethyl fumarate, Natalizumab. Patient expenditure for informal care and community services were the predominant public costs, followed by disease management costs. For active treatment, DMT costs were approximately the second highest expenditure category. Neuberger 2021: data from a survey have been used for evaluate work and activity impairment in patients with MS treated with ocrelizumab (OCR) versus other disease-modifying therapies (DMTs). The evidence suggests that patients with MS treated with OCR experience lower work and activity impairment than patients treated with other DMTs Bonafede 2021: reported the results of a retrospective, administrative claims-based US study that examined productivity loss and associated costs among patients with MS initiating a DMT compared with matched non-MS controls and the indirect burden and cost by route of administration of DMT. When DMT oral and injectable users were compared, their absenteeism and short-term disability productivity loss and costs were generally similar in the first calendar year. Patients initiating oral DMTs had less than half the number of days on long-term disability than patients initiating injectable DMTs. Other measures of productivity were similar between route of administration. Atlas of MS clinical management 2021. A global survey on the availability of resources and services for people with MS in different regions of the world found a widening gap between high- and low- income countries in the access to DMTs. They found that 72% of countries cite barriers to accessing DMTs. Globally the most common barrier is the cost to the government, healthcare system or insurance provider, which is cited by experts in around half of all reporting countries. In addition to cost, experts in low income countries often report both a lack of healthcare professionals and a lack of knowledge of DMTs amongst professionals as a barrier to accessing therapies. -Off-label status No evidence was found. -Mode of administration, frequency and storage of DMTs No evidence was found. -Requirement to attend a healthcare facility for administration and/or follow-up monitoring No evidence was found CONSIDERATIONS FOR CLINICIANS -Cost Duddy 2021: explored the real-world management of SPMS in the UK. Healthcare professionals involved in the management of patients with SPMS from geographically distributed MS neurology centres in the UK participated in face-to-face or telephone interviews. Regarding DMTs management, approximately two-thirds of the respondents reported they followed a specific guideline for DMT management, most of whom followed the NHSE algorithm. Reasons reported by respondents for not using DMTs on some patients with confirmed SPMS included: funding/reimbursement mediated restrictions, absence of active inflammation and/or relapse, lack of treatment effectiveness, patient eligibility and an unfavourable risk-benefit analysis. - Access to therapy Narayanan 2014: survey aimed to assess health care provider (HCP) perception of barriers to prescribing medications to patients with Multiple Sclerosis (MS) in EU and the US. METHODS: HCP perceptions of the following barriers to prescribing interferons (all types), glatiramer acetate, natalizumab and fingolimod were assessed: patients prefer other medications (barrier-1), availability/cost (barrier-2), guidelines/license restrictions (barrier-3) and drug-related issues (barrier-4). Drug-related issue was the most frequently cited barrier to prescribing MS medications both in EU and the US. Drug availability/cost and guidelines/license restrictions were more often cited by HCPs in the US and 5EU respectively. See table below:  Off-label status No evidence was found. -Mode of administration, frequency and storage of DMTs No evidence was found. -Requirement to attend a healthcare facility for administration and/or follow-up monitoring No evidence was found. CONSIDERATIONS FOR CLINICIANS AND PAYERS -Cost Filippi 2022: reviewed the evidence and the professional experiences from clinical healthcare professionals and payer advisors, on the importance of providing early and unrestricted access to high efficacy DMTs (HE-DMTs), such as fingolimod and natalizumab, alemtuzumab, ocrelizumab, and ofatumumab. From a patient perspective early access to novel HE-DMTs with a positive benefit–risk profile could improve their long-term outcomes. From a budget impact perspective, the availability of HE DMTs with a positive risk/benefit profile and a reasonable price proposition allows for their use early in the course of the disease, which would positively impact affordability, health care sustainability and cost savings. From a clinician perspective early and unrestricted access to HE DMTs would provide the freedom of choice of an appropriate treatment by expert physicians. Even though there is a need for long-term, real-world safety data, this should not be the reason to restrict access to novel HE DMTs, as this would potentially translate to 5- to 10-year delayed access. KEY POINTS · People with MS in different regions of the world have to pay some or all of the cost of their DMTs, ranging from 39% of countries in Europe to 76% of countries in the Americas. · Global problems with the continuous provision of DMT treatment due to an irregular supply of DMT or for reimbursement renewed or need to take regular tests to prove continued eligibility. · Surveys show that drug-related problems (circumstance involving drug therapy that actually or potentially interferes with desired health outcomes) issue is the most frequently cited barrier to prescribing MS medications both in EU and the US. · From a clinician and payers perspective, the availability of high efficacy DMTs with a positive risk/benefit profile and a reasonable price positively impact affordability, health care sustainability and cost savings. References - Kotsopoulos N, Connolly MA-OX, Dort T, Kavaliunas A. The fiscal consequences of public health investments in disease-modifying therapies for the treatment of multiple sclerosis in Sweden. 2020(1941-837X (Electronic)). - Neuberger EE, Abbass IM, Jones E, Engmann NJ. Work Productivity Outcomes Associated with Ocrelizumab Compared with Other Disease-Modifying Therapies for Multiple Sclerosis. Neurol Ther. 2021 Jun;10(1):183-196. - Filippi et al. Early and unrestricted access to high-efficacy disease-modifying therapies: a consensus to optimize benefits for people living with multiple sclerosis. J Neurology 2022;269:1670–1677 - Bonafede M, Mehta R, Kim G, Sruti I, Tian M, Pelletier C, Goldfarb N. Productivity Loss and Associated Costs Among Employed Patients Receiving Disease-Modifying Treatment for Multiple Sclerosis. Pharmacoecon Open. 2021 Mar;5(1):23-34. - Duddy M, Wilkinson C, Medhurst S, Rhys K. Results from SPECTRUM: A survey of healthcare professionals to understand current diagnosis and management practices for secondary progressive multiple sclerosis in the United Kingdom. Mult Scler Relat Disord. 2021 Oct;55:103174. Narayanan, S. Khan, H. Gabriele, S. White, J. Barriers to prescribing medications to patients with multiple sclerosis: A comparison of health care provider perceptions in European union (EU) and the United States, Value in Health; 2014; 17(3): A66 Protocol: https://osf.io/5edjf | Feasibility of implementation is affected by resource requirements. MSIF has provided several pathways for affordability in criteria 7 'resource requirements'. On-label/off-label status may be relevant to feasibility as linked to (a) current availability and (b) other organisations doing access initiatives, e.g. pre-qualification and push for rituximab for cancer by WHO and CHAI. There is a lack of evidence on feasibility and Atlas insight on DMTs used may be relevant. Consideration of feasibility for all key stakeholders is important. Please refer to feasibility assessment by expert input spreadsheet for information on mode of administration, frequency of administration, storage, required and optional pre-tests and monitoring and feasibility assessment from Malaysia and Zambia: Cold-chain, healthcare infrastructure (e.g. infusion suites), access to pre-tests and monitoring all affect feasibility. ECG and OCT sometimes only available at national referral hospitals. Feasibility of fingolimod and siponimod depends on access to testing in particular countries/locales. Use of siponimod requires mandatory genotyping, which is not available in many regions. Natalizumab requires JCV testing due to risk of PML, but the testing is not available in some settings. Concern for rebound disease if lose access to natalizumab, fingolimod or siponimod. The panel noted that feasibility for siponimod and natalizumab varies depending on the monitoring available and reliability of supply. Feasibility of siponimod (varies) and fingolimod (probably yes) differs due to the genetic testing required pre-treatment. Fingolimod requires six-hour monitoring and ECG before and after first dose. ECG is more available than the genetic testing and monitoring for six hours may not be an issue, whereas the testing is simply not available in some settings. Fingolimod monitoring is burdensome but more feasible than the genetic testing. Azathioprine already widely used in low resource settings for many conditions. Genetic testing is ‘recommended’ not ‘required’. Azathioprine is feasible, depending if you follow genetic testing guidance. Also does not require refrigeration. Immunoglobulins are incredibly expensive, require IV infusion with careful monitoring for renal dysfunction. This makes then unfeasible in a number of settings. In the real-world setting used with poor results in PMS, with side effects and high cost. They require day care, an infusion nurse and time as the infusions take half a day. For immunoglobulin the panel discussed whether it should be judged as ‘varies’ as the use of immunoglobulin in high income settings is feasible, similar to what the panel discussed for natalizumab and alemtuzumab. If used, the medicine is to some extent feasible, but it was noted that it was rarely used in the Atlas data and several panel members noted that it was not or very rarely used in high income settings for MS. However, immunoglobulins are used for other conditions in high income settings. The panel judged ‘probably no’ for immunoglobulin feasibility. Using the spreadsheet prepared and trying to separate out cost from feasibility, the panel suggested the following judgements: Yes: azathioprine, methotrexate Probably yes: fingolimod, ocrelizumab, rituximab, interferons, GA (monitoring, infusion and cold-chain) Varies: siponimod, natalizumab (monitoring, genetic screening, JCV/PML and cold-chain) Probably no: immunoglobulin. The panel revisited judgement of fingolimod ('probably yes') after discussing feasability of fingolimod in RMS, specifically linked to rebound effect. The panel noted that any rebound effect would be less of a concern if not having relapses. Panel agreed to keep fingolimod as ‘probably yes’ for PMS but judge ‘varies’ in RMS as rebound is a higher risk for RMS. | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
AvailabilityWhat is the regulatory status, market availability, and availability of pharmacopoeial standards for this medicine? | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Judgement | Research evidence | Additional considerations | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
No systematic review was performed for availability. The clinical management module of Atlas of MS (2021) collected data through a systematic survey on which DMTs were used in each country around the world in 2019/2020. Usage is a proxy for availability. No country reported laquinimod or steroids use as a DMT.  Availability of on-label and off-label DMTs were analysed on 137 national essential medicines lists (EML) from the WHO national EML database (Laurson et al. 2021, MSJ). Listing on a national EML is a proxy for availability but in some countries, medicines can be available and reimbursed, despite not being listed on the national EML (e.g. Egypt). In other instances, medicines may be listed and prioritised, but still not continuously available in the clinic due to budgetary and other challenges. The analysis did not include immunoglobulin, laquinimod, siponimod or steroids.  | The panel considered availability across global settings surveyed in the MSIF atlas. Rituximab, azathioprine, methotrexate and interferon are already listed on the WHO EML. Methotrexate not extensively used for MS according to Atlas of MS (41/107), but listed on 126/137 on national EMLs. Methotrexate is on the WHO EML for other conditions so it should be available in many countries. On the WHO EML for: Acute lymphoblastic leukaemia, Acute promyelocytic leukaemia, Burkitt lymphoma, Early stage breast cancer, Gestational trophoblastic neoplasia, Osteosarcoma. Siponimod was approved 2019 (US FDA) and 2020 (EMA) - Atlas data collected 2020. Availability most likely affected by this. Immunoglobulin is used only in three countries around the world for MS, according to the Atlas. Two high income countries and one upper middle income country, it is probably the least available DMTs. Glatiramer acetate, ocrelizumab and natalizumab are more available in HICs and UMICs, and were judeged as 'varies'. Panel judgements: Available in most settings: Interferon beta 1a, interferon beta 1b, fingolimod, rituximab, azathioprine, methotrexate Probably available in most settings: Probably not available in most settings: siponimod (new DMT), immunoglobulins Varies: GA, ocrelizumab, natalizumab | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Summary of judgements
| Azathioprine | Fingolimod | Rituximab | Ocrelizumab | Glatiramer acetate | Immunoglobulins | Interferon Beta 1a (Avonex Rebif) | Interferon Beta 1b | Methotrexate | Siponimod | Natalizumab | |
|---|---|---|---|---|---|---|---|---|---|---|---|
Desirable Effects | Large | Moderate | Moderate | Moderate | Moderate | Moderate | Large | Moderate | Large | Large | Moderate |
Undesirable Effects | Trivial | Trivial | Trivial | Trivial | Trivial | Trivial | Moderate | Small | Trivial | Trivial | Trivial |
Certainty of evidence | Very low | Low | Very low | Very low | Very low | Very low | Low | Very low | Very low | Low | Very low |
Values | Probably no important uncertainty or variability | Probably no important uncertainty or variability | Probably no important uncertainty or variability | Probably no important uncertainty or variability | Probably no important uncertainty or variability | Probably no important uncertainty or variability | Probably no important uncertainty or variability | Probably no important uncertainty or variability | Probably no important uncertainty or variability | Probably no important uncertainty or variability | Probably no important uncertainty or variability |
Balance of effects | Probably favors the intervention | Probably favors the intervention | Probably favors the intervention | Probably favors the intervention | Probably favors the intervention | Probably favors the intervention | Probably favors the intervention | Probably favors the intervention | Probably favors the intervention | Favors the intervention | Probably favors the intervention |
Resources required | Moderate costs | Large costs | Large costs | Large costs | Large costs | Large costs | Large costs | Large costs | Negligible costs and savings | Large costs | Large costs |
Cost effectiveness | No included studies | No included studies | No included studies | Varies | Varies | No included studies | Varies | Varies | No included studies | Varies | No included studies |
Equity | Probably increased | Probably reduced | Probably increased | Probably reduced | Probably no impact | Reduced | Probably no impact | Probably no impact | Probably no impact | Probably reduced | Probably reduced |
Acceptability | Yes | Probably yes | Probably yes | Probably yes | Probably yes | Probably no | Probably yes | Probably yes | Yes | Probably yes | Probably yes |
Feasibility | Yes | Probably yes | Probably yes | Probably yes | Probably yes | Probably no | Probably yes | Probably yes | Yes | Varies | Varies |
Availability | Varies | ||||||||||
Conclusions
Recommendation(s) |
The MEMP suggests for in priority order (conditional recommendation): 1. rituximab (very low certainty ⊕OOO), 2. glatiramer acetate (very low certainty ⊕OOO), 3. ocrelizumab (very low certainty ⊕OOO) 4. interferon beta 1a (low certainty ⊕⊕OO), 5. fingolimod (low certainty ⊕⊕OO), 6. interferon beta 1b (very low certainty ⊕OOO) for active and/or progressing progressive forms of MS. Remark: The recommendation is conditional due to low and very low certainty of evidence. Justification: Rituximab is a feasible and acceptable option in low-resource settings due to balance of effects, mode of administration (6-monthly infusions), low maintenance for screening and monitoring with low risk of rebound effect if treatment is discontinued, and low discontinuation rate, but requires infusion facilities and cold storage at the healthcare facility. Glatiramer acetate is a feasible and acceptable option in low-resource settings due to balance of effects, very low maintenance for screening and monitoring, but is less acceptable due to mode and frequency of administration (injection), and requirement of cold-storage by person with MS. Ocrelizumab is a feasible and acceptable option in low-resource settings due to balance of effects, low maintenance for screening and monitoring, low discontinuation rate, mode of administration (6-monthly infusions), but requires infusion facilities and cold storage at the healthcare facility. It is less acceptable than rituximab due to significant cost of the medication. Interferons beta 1a and 1b are feasible and acceptable options in low-resource settings due to balance of effects, low maintenance for screening and monitoring, but are less acceptable due to mode and frequency of administration (injection), requirement of cold-storage by person with MS and type of adverse events. Fingolimod is a feasible and acceptable option in low-resource settings due to balance of effects, mode of administration (oral), easy storage, but requires more maintenance for screening and monitoring, and has a risk of rebound of MS disease activity if access to treatment is discontinued suddenly, e.g. due to unreliable supply of medicine. The MEMP suggests either for or against in priority order (conditional conditional and neutral recommendation, dependent on setting): 1. siponimod (low certainty ⊕⊕OO), 2. natalizumab (very low certainty ⊕OOO), 3. immunoglobulins (very low certainty ⊕OOO) for active and/or progressing progressive forms of MS. Remark: Feasibility of pre-tests, monitoring requirements, cost and affordability are concerns limiting the application of these DMTs in some low-resource settings. The panel felt a recommendation either for or against these medicines for low-resource settings was appropriate, despite evidence of clinical benefit. Immunoglobulin use was noted to be rare even in high-income settings, with efforts to reduce demand for immunoglobulin in many countries. Justification: The panel noted that the evidence on balance of the effects clearly favours siponimod and natalizumab. Despite the demonstrated benefit, the panel noted variable feasibility issues for low-resource settings in the access to and cost of pre-screening and monitoring required, e.g. for siponimod CYP2C9 genotyping and for natalizumab regular JCV testing and MRI monitoring for PML. These tests are essential for the safe use of these DMTs and not widely available in low-resource settings. It was noted that the high cost of medicines resulted in a significant budget impact. Natalizumab and siponimod were noted to be used routinely in high-income settings, whereas the use of immunoglobulin was rare. The MEMP suggests for in priority order (conditional recommendation): 1. azathioprine (very low certainty ⊕OOO), 2. methotrexate (very low certainty ⊕OOO) in clinical settings where no alternative treatments are accessible for active and/or progressing progressive forms of MS. Remark: This recommendation is conditional to other treatment options not being accessible due to the very low evidence-base available. Use in research settings may also be appropriate due to the need for higher quality evidence for these medicines, although trials with placebo would be considered unethical. Justification: Azathioprine and methotrexate have a conditional recommendation for with a condition of no alternative DMTs being accessible, where the alternative would be no treatment. This condition was due to the evidence-base being very limited and more research would be required to ascertain effects of these DMTs in progressive forms of MS. The DMTs are oral treatments, widely available in health systems with a low cost, not requiring cold-chain, making them a feasible option in low-resource settings. The ranking is based on balance of effects. |
Justification |
Subgroup considerations |
The MEMP panel assessed evidence for progressive MS populations overall. The panel noted most evidence informing this assessment was from active and/or progressing PMS. The panel added subgroup considerations for the following populations: Not active and not progressing or indeterminate forms of PMS: The panel suggested the benefit/harm ratio may be different in this population as evidence suggests DMTs are most effective in active populations. The panel suggests discussion with pwMS about the benefits/harms of different treatment options depending on their personal circumstances and individualized decisions about whether or not to take DMTs made in conjunction with their clinicians. Active and/or progressing forms of PMS when there is a lack of treatment response: No randomised-controlled trial evidence was available to MEMP to inform specific recommendations for active and/or progressing PMS when there is a lack of treatment response. Consideration may be given to results of observational studies and individual circumstances including how rapidly MS is progressing, age, symptoms, disability, comorbid diseases, risk of infection and concomitant medication in the decision to try a different medicine based on the accessibility of medicines in the setting. |
Multiple Chronic conditions and Polypharmacy |
Consideration of concomitant medication and polypharmacy is important for pwMS, and MS DMTs should be frequently re-evaluated as pwMS age, develop new comorbidities, and begin new medications. |
Clinical considerations |
For all DMTs the following infection screening is recommended: TB, HIV, Hep C, Hep B, VZV and syphilis. In addition, the following tests and monitoring are needed: |
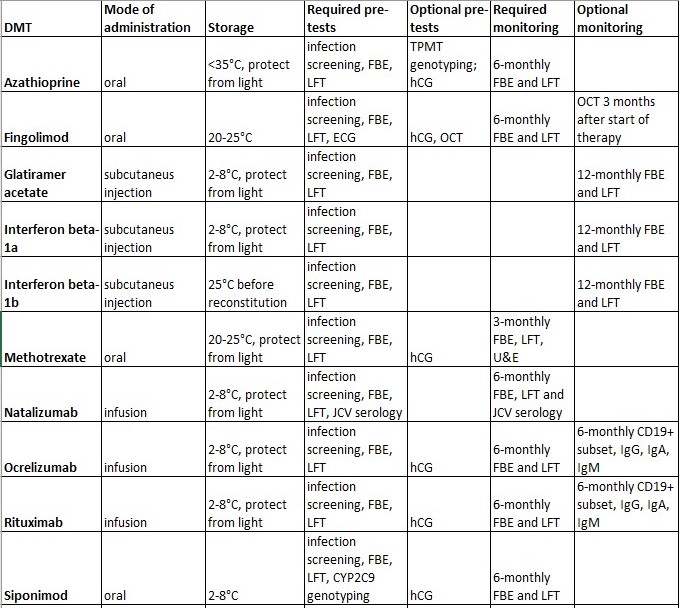{kind=link}
Research priorities |
MEMP suggests prioritizing research on: 1. Systematic review of non-randomised controlled studies for all DMTs to further inform comparative effectiveness. 2. Improving the evidence-base for medicines that are off-label and have follow-on products available, and therefore are more accessible, e.g. rituximab, azathioprine and methotrexate. 3. Evaluating long-term risks and benefits of siponimod as it finds more widespread use in larger populations. |